
Lots of books are published each year, and I can only read a few of them. But, when a really important general interest book comes along, I often put it on the top of my “to be read” pile. In September, Dr. Marty Makary, a surgeon associated with Johns Hopkins, released a book entitled The Price We Pay: What Book American Healthcare—And How to Fix It. Since most people in America eventually get sick or have an accident, and only a few of us are fifty rich, this is the ultimate general interest book.
In Part I, entitled “Gold Rush” Makary doesn’t have to travel far—he visits “health fairs” at local churches, where salespeople disguised as medical professionals do screening tests and scare participants, mostly those on Medicare, into unnecessary and rather expensive procedures, such as placing stents into leg veins. In the second chapter, he discusses the lack of transparency in hospital pricing, as well as the astronomical rise in common procedures. For instance, a medical center in New Jersey offers joint replacement surgery for $135,400.00, which rose a mere 76.8% in a single year. BTW, Medicare only pays 13K for that procedure. For his third chapter, Makary travels to Carlsbad, NM, where the medical center seems to have overcharged and then sued almost everyone in town. Back in Virginia, Makary visits the courthouse to learn more about similar shenanigans at Mary Washington Hospital in Fredericksburg. Sadly, this hospital is supposed to be a “not for profit” hospital, and thus receives favored tax status, too. Also in this section, Makary provides an analysis of the proliferation of for profit helicopter ambulance services, which charge somewhere between $40K and $60K for a ride that I could make in an hour in my Toyota.
In the second portion of the book, Makary delves into some medical practices that can be improved by focusing on individual physicians. One OB doctor in Florida had a reasonable rate of C-sections, until figuring in Fridays, when the rate rose 80%. Why? The good doctor didn’t want to be bothered on the weekend, so moms who were in labor on Friday got the surgery. This section of the book also discusses the opioid crisis, and Makary admits that he had to learn to write fewer prescriptions for pain pills, after learning about the misuse of all those pills.
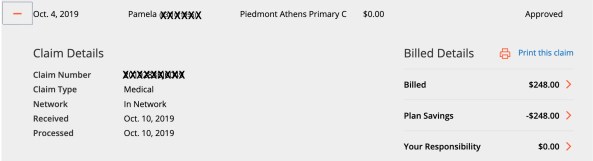
Part III of the book is about “Redesigning Healthcare” and it does offer several solutions to problems, but one chapter in this section explains how drug prices are affected by middle men (pharmacy benefits managers) who don’t supply anything other than a big bill for their services. Here’s an example: A pharmacy is paid $34.94 for 90 40mg doses of Zocor, but the employer is charged $442.85–and the PBM gets over $400 on that one transaction. Another chapter discusses problems in health insurance, which less and less helpful except in catastrophic circumstances, and there is even a chapter on “wellness” and how those well meaning programs are far too costly, especially as they often mean an invasion of privacy, or worse, over-treatment for minor issues.
Makary doesn’t make the mistake of only discussing problems without discussing solutions. Several positive programs are mentioned throughout the text, including websites such as ImprovingWisely.com, and the last chapter is a bit of a call to arms. In short, legislators and employers need to be educated on these matters, and healthcare consumers should do everything possible to demand transparent pricing for upcoming procedures.
The Price We Pay is a very important book. This should be the topic of your next book club, a gift for your friends and/or family, or even a holiday gift for your doctor or your legislator. Please buy this book, read it, and pass it on. Knowledge is power, and as this text has lots of information for Americans, this may well be the most important book you will read this year.
 Like many people in the USA, I am concerned about the state of our health care. Don’t get me wrong, I’m grateful to live in a country that has lots of great medical facilities and practitioners. But, I’ve watched people go through some pretty difficult situations, too, so I read
Like many people in the USA, I am concerned about the state of our health care. Don’t get me wrong, I’m grateful to live in a country that has lots of great medical facilities and practitioners. But, I’ve watched people go through some pretty difficult situations, too, so I read 